

Caldwell Luc surgery
Introduction:
Caldwell Luc surgery is approximately 120 years old. This surgery till recently was an
important tool in the armamentarium of an Otolaryngologist. Now the indications for this
procedure is getting fewer and fewer with Endoscopic sinus surgery becoming common.
The fundamental concept of this surgical approach is to replace the diseased / scarred
mucosa from maxillary sinus with a new one. This is easily said than done. It is fairly simple
to remove diseased mucosa. New mucosa replacement is dependent on the regenerative
capacity of the patient.
This approach can also be used to access adjacent areas, which could be difficult to access
otherwise. This procedure is not without its own set of complications. It is imperative on
the part of the surgeon to weigh in the benefits vs complications before advising the
patient.
Description of paranasal sinuses have been traced up to the 16th century. Berenger Del
Carpi an anatomist first described the existence of paranasal sinuses and also infections
involving this area. Detailed description of maxillary sinusitis was first provided by Nathaniel
Highmore. Maxillary sinuses hence bear the name “Antrum of Highmore”. He first
attempted to drain the infected sinus cavity by inserting a silver needle (bodkin) through an
empty tooth socket. By doing this he was able to enter into the maxillary sinus cavity and
was able to drain infected pus from it. Many surgeons used this approach to drain maxillary
sinuses. It was Lamorier in 1743 and Desault in 1798 who successfully demonstrated that
maxillary sinus cavity could be approached via the canine fossa route. According to them
this was the weakest portion of all its boundaries.
In 1835 John Hunter popularized intranasal antrostomy via the inferior meatus. George W
Caldwell of New York combined both canine fossa approach and inferior meatal antrostomy
with success in managing patients with maxillary sinusitis. This work became a sensational
publication in 1893 (New York Medical Journal). A similar procedure was routinely
performed in France by Henry Luc in 1897. Only difference between their two procedures
was that Luc performed intranasal antrostomy via the middle meatus while Caldwell
performed inferior meatal antrostomy via the inferior meatus.
Better understanding of mucociliary clearance mechanism has popularized conservative
surgical procedures like:
Fess
Mini Fess
Balloon sinuplasty
It should be stressed that Caldwell Luc procedure provides the maximum exposure of
maxillary sinuses, floor of orbit and pterygopalatine fossa.
Indications:
1. Mycotic maxillary sinusitis
2. Multiseptate maxillary sinus mucocele
3. A/C polyp (Recurrent)
4. Oroantral fistula
5. Revision procedures
6. Access for transantral sphenoidectomy, orbital decompression, orbital floor repair,
exploration of pterygoplatine fossa
7. Excision of tumors involving the antrum (inverted papilloma)
8. Visualization of orbital floor during orbital floor decompression surgeries
9. Removal of foreign bodies from maxillary antrum
In patients with severe mucociliary irreversible damage (Kartagener’s syndrome, Young’s
syndrome) this could be the only approach to drain infected material from maxillary sinuses.
Procedure:
This surgery can be performed either under LA/GA.

Image showing canine fossa marked in a skull
The maxillary sinus is lined by ciliated columnar epithelium. The cilia beats towards the
natural ostium thereby moving the secretions towards the natural ostium. Hence inferior
meatal antrostomy does not ensure drainage of the sinus in the presence of normal ciliary
beat.
The adult maxillary sinus is about:
25-35 mm wide
36-45 mm high
38-45 mm long
Its average volume is about 15 ml /(one fluid ounce).
Superior wall of maxillary sinus – orbital floor. This sometimes can be dehiscent. The
infraorbital nerve is on the roof of the sinus. Medially and posteriorly the roof is composed
of the floor of the ethmoid sinuses.
Anterior wall of maxillary sinus – This wall contains the nerves and vessels that supply the
upper teeth. This wall is thinner anteriorly and it thickens posterolaterally where it joins the
zygomatic process. Septae are present anteriorly in about a third of the cases.
Medial wall – This wall separates maxillary sinus from nasal cavity. The inferior turbinate is
attached along the nasal wall below the level of maxillary sinus ostium. The nasolacrimal
duct traverses the thicker bone at the junction of medial and anterior walls and it opens into
the nose below the inferior turbinate in the middle meatus. Maxillary sinus communicates
with the nasal cavity via the maxillary sinus ostium in the hiatus semilunaris of the middle
meatus.
Posterior wall – This is formed by the infratemporal surface of the maxilla and it separates
the sinus from the pterygomaxillary fissure and the pterygopalatine fossa. Pterygopalatine
fossa contains the internal maxillary artery and its branches, pterygopalatine ganglion and
its branches.
The dimensions of maxillary sinus cavity changes with age and could affect the surgery as
the anatomy gets changed with age. The sinus expands at the rate of 2-3 mm / year and this
process continues till adulthood. At birth maxillary sinus is rather small and its floor lies 4
mm above the floor of the nasal cavity. At the age of 9 the floor of the maxillary sinuses is
at the same level as that of the nasal cavity. Their dimensions being 2x2x3 cms. In adults
the sinus floor is 0.5 – 1 cm below that of the nasal cavity. The alveolus of maxilla atrophies
in edentulous patients and the floor in these patients could be still lower.
Anatomy of the canine fossa:
The canine fossa is the thinnest portion of the anterior wall of the maxillary sinus. Hence it is
easy to breach this area and enter into the sinus. Boundaries of the canine fossa include:
1. Canine eminence formed by the canine tooth – medial
2. Root of the zygoma – laterally
3. Alveolar process of maxilla - inferiorly
4. Infraorbital foramen with the infraorbital nerve superiorly
Infraorbital foramen:
This foramen transmits infraorbital nerve, artery and vein. The infraorbital neurovascular
bundle traverses a groove in the orbital floor which happens to be the roof of maxillary
sinus. This area can also be dehiscent in some individuals. The neurovascular bundle exits
via the infraorbital foramen which is located approximately 5 mm below the midportion of
the inferior orbital rim to enter the soft tissues of the cheek. Branches of this nerve supply
the lower eyelid, nose, cheek, and upper lip. Care should be taken while elevating the
periosteum from the anterior wall of maxillary sinus to avoid injury to this nerve. Branches
of anterior and posterior superior alveolar nerves traverse through the bone to supply
upper teeth and gums. There is risk of injury to these nerves when antrostomy is extended
too low. Injury to these nerves could cause loss of sensation of upper dentition and gums.
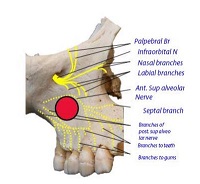
Infraorbital nerve and its branches
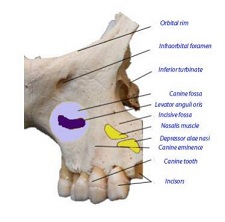
Anatomy of canine fossa along with its boundaries
It should be pointed out that no significant blood vessels are encountered during this
surgical procedure with the exception of small infraorbital vessels that exit from the
infraorbital foramen. Significant bleeding is possible only when one breaches the posterior
wall of the maxilla and enters the pterygopalatine fossa where internal maxillary artery can
be encountered.
Patient preparation:
Patient should be placed in recumbent position with head slightly elevated. Nasal cavities
are packed with cotton pledgets dipped in 4% xylocaine with 1 in 100,000 adrenaline. These
pledgets should be squeezed dry before insertion. This is because the critical toxic dose of
xylocaine in this concentration is about 7 ml. On no account this amount should be
exceeded.
Under direct illumination pledgets are placed in Inferior meatus, floor of the nasal cavity and
in the middle meatus area. At least 10 – 15 minutes interval should be given for the drug to
take its effect.
If the surgery is planned under local anesthesia then one more cotton pledget soaked in 4%
xylocaine adrenaline mixture and is placed in the sublabial area on the side of surgery. This
is done to anesthetize the mucosa over canine fossa.
Infiltration local anesthesia is preferred in this scenario. About 1 ml of 2% xylocaine mixed
with 1 in 200,000 adrenaline is infiltrated over the canine fossa area. Since the mucosa over
the canine fossa would have already been anesthetized by the cotton pledget soaked in 4%
xylocaine the process of infiltration would invariably be painless. This infiltration blocks the
inferior orbital nerve and its branch anterior superior alveolar nerve. The patient is also
mildly sedated to alleviate the anxiety.
If general anesthesia is preferred then the patient should be positioned only after the
anesthetist has intubated the patient.
Incision:
Incision is given in the Bucco gingival sulcus. The length of the incision could be about 3 - 4
cms. Ideally the incision is begun at the canine eminence and should run laterally.
Langenbachs retractor is used to retract the mucosal and soft tissue to expose the anterior
wall of the maxilla.

Image showing sub labial incision being given
The retractor should be applied in such a way that it should not cause excessive traction to the soft tissue in the area. Excessive traction if applied can lead to excessive cheek oedema post operatively which could take about a week to subside completely.

Image showing Langenbeck retractor being applied
In the next step a periosteal elevator is used to elevate the periosteum from the anterior wall of maxillary sinus till the infraorbital foramen becomes visible. Care should be taken not to damage infraorbital neurovascular bundle.

Periosteal elevator seen being used to elevate periosteum from the anterior wall of maxilla
Anterior wall of maxillary sinus antrum is opened up using a gouge and hammer or by cutting it using a cutting burr. The size of the antrostomy should be 1.5 – 2 cm in diameter and more or less circular. Instruments can be introduced via the antrostomy and the diseased mucosa can be curetted out under direct vision. The entire maxillary sinus cavity is directly visible through the antrostomy opening. Of course, there could be some blind spots which may not be fully visible i.e. the anterior wall and the antero lateral portion of the sinus cavity. A wide angled nasal endoscope can be introduced via the antrostomy opening to visualize even these hidden areas. If the pterygopalatine fossa needs to be approached then the posterior wall of the maxillary sinus antrum should be breached using gouge and hammer or a cutting burr.
Creation of naso antral window in the inferior meatus:
This process helps in removal of antral pack after surgical procedure. Visualization of antral cavity is possible through this opening. Miles retrograde gouge is used for this purpose. This gouge has a unique curvature which will enable it to slide into the inferior meatus.

The gouge is held in the dominant hand with index finger serving as a guard to control the perforation process. The gouge is slipping into the inferior meatus. As soon as it hinges in the lateral nasal wall the medial wall of antrum is perforated at the junction of anterior third and posterior 2/3 of inferior meatus. Its unique tip ensures that it holds the bone fragment after perforation is made on withdrawal. Medicated nasal pack can be introduced via the inferior meatal antrostomy using long-curved forceps and delivered into the maxillary antrum via inferior meatal antrostomy. One end of the ribbon gauze used to pack the antrum is brought out via the inferior meatal antrostomy making their later removal via the nasal cavity that much easier. Mucosal wound is closed using 3-0 chromic catgut. The antral pack can be removed via the nasal cavity after 48 hours as it is accessible through the inferior meatal antrostomy.

Image showing canine fossa antrostomy

Antral mucosa visible through antrostomy

Wound closure seen
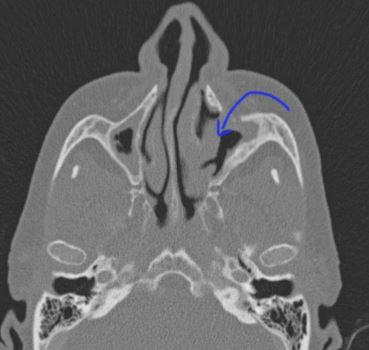
Arrow showing Caldwell Luc surgery opening in the canine fossa
Post-operative care:
1. Ice packs can be used over cheek to reduce oedema and discomfort
2. Nasal and antral packing can be removed between 24-48 hours
3. Nose blowing is avoided as it could cause emphysema of cheek area
4. If patient uses denture then it should not be worn for at least a week to facilitate mucosal healing
Complications:
1. Oedema over cheek – This can happen if retraction of soft tissue in the area was firm and not gentle. Sometimes subcutaneous emphysema can develop due to leakage of air from the antrum into the subcutaneous tissues of cheek. This complication is self-limiting and will reduce within a week.
2. Injury to infra orbital nerve causing anesthesia of upper teeth and lateral wall of nose. It can even cause pain and numbness over the face
3. Injury to nasolacrimal duct while performing inferior meatal antrostomy
4. Devitalization of teeth due to injury to its root